Section 136 - exposure
Section 136: When Mental Health Becomes Criminal - and a Race Issue
Corridors rammed, trolley’s lining the halls, seats strewn like an incomplete jigsaw and dotted with a pick ‘n’ mix of injuries and illnesses. The recognisable blanket of sound washes the room with screams, noisy baby chatter, whimpering patients, rowing partners, drunken blabber, and nervous panic. The impactful hot smell of queasy bodies, displeased tapping feet, phones jingling with urgency, and the rhythmic sighs partner the steady, constant beep of cardiac monitors as an anxious reminder of possible death next door. The clock possesses the audience. This is 12:00AM in Manchester Royal ED in the UK, the wait is a grave 8 hours. Suddenly, a young Irish man explodes into the room and with bullish momentum dives to the floor half-exclaiming “Up the Ra!” as the doors swing on a panicked pendulum behind him. His forehead has a chip missing causing his face to be stained ruby. He enters a fidgety state of unconsciousness and the audience go back to clock-watching. A&E is an uncontrollably hectic place that most members of the public cannot bear to endure in sound mind, and the thought of experiencing this during a state of heightened mental distress, is disturbing.
Just when your mental health reaches the lowest point imaginable…you have an audience to watch it unravel. This can be the reality of Section 136. “It’s inhumane”, explains Alison McKillop, a former 136 detainee, “there was a time I was handcuffed to a bed…they tied my feet up to restrain me. I began to bang my head against the wall next to me, I wasn’t myself”. She looks back to late 2025, “you sit on a chair for 12 hours with the police stopping you from leaving. It's horrible when you’re stressed…the hospital goes by thinking you’ve done something bad”. The image of police officers detaining a person in a place of derailment can easily draw the attention of a time rich crowd.
“It’s stressful to watch when people come in having tried to kill themselves and have nowhere else to go so are forced to sit either in A&E or what we call a security room, which is just an old cupboard with a chair”, sighed Caitlin Williams, an NHS nurse, the statement loaded with understandable exasperation. Another former 136 detainee mirrored, “In my experience I’ve been cuffed most of the time as well, I get it, but it makes you feel like a criminal when you’ve not done any criminal activity”. In your most vulnerable state awaits security cupboards, bustling environments, and a judgemental crowd. Your mental decline and the officers to accompany it becomes entertainment for the night.
Section 136 of the Mental Health Act is for members of the public displaying signs of mental distress and in need of immediate care1. This is specifically intended for the police to remove the person from any public space and take them to a place of safety. The first port of call is to be a health-based place of safety (HBPoS), specifically designed for mental health crisis2. Alternatively, A&E can be used when the person requires urgent medical attention. Individuals can be detained for up to 36 hours to receive a rapid mental health assessment from professionals. It is recognised that A&E is not a suitable environment for Section 136 patients, especially children, due to the non-mental health specific care available3. In 2025, A&E saw up to 77,000 people per day, these numbers remove any notion of privacy for those in breakdown. However, “there never is any place for them to go so they come to us, so many more are on 136 now than ever in A&E”, says Rachel Eastwood, an A&E nurse, her frustration ticked. Is this the reality across the UK?
The use of A&E as a place of safety has slowly crept up, pressing additional strain on the overloaded NHS, responsible for 8% of 136 patients in 2017 and tipping the scale at 51% as of 20254,with HBPoS use declining. It is estimated there are 160 HBPoS across England and Wales5 to accommodate the yearly increase in mental health, and yet this number goes unmonitored despite 60% of ICB’s feeling numbers are not suitable2. The closure of HBPoS across London6 and limited numbers7 across the UK has been problematic for staff and potentially traumatic for the mentally unwell. “There should be more 136 suites so they can have their own space and time within a mental health facility, but these are never free”, Eastwood says, referring to the situation she experiences on a daily basis.
The Royal College of Nursing has lobbied against A&E being used as an appropriate place of safety nevertheless, more than 1.3 million people have presented to A&E in the last 6 years in mental distress8. A response from NHS England obtained for this investigation found that the average waiting time between 2023-2025 for children was 16.9 hours under s136 in A&E and 5% of children waited just under 3 days in a deteriorating mental state. Further information uncovered adults waiting 12.6 hours on average under s136, with 5% spending over 41 hours. “I’ve waited three days before under section 136, the waiting is horrible when you’re like that, just waiting for a bed or something to happen”, the former patient looked back on her time in continued torment.
Regional variety is clear yet most children are taken to A&E first (77% in London; 83% in the Northern areas9), with waits of up to 18.5 hours, but review finds shorter waits are available in areas with better access to a HBPoS. However, it’s apparent that there is no consistent recording of children waiting in A&E in mental crisis and no monitor of how many HBPoS are needed and failing to be staffed.
National statistics do not break down adult and children s136 locations, and records held by ICB’s, hospital trusts, and police are often inconsistent. West Yorkshire police had 1,086 unrecorded locations for s136 in 2024/2510, leaving some children untraced. A social worker in the Leeds area, kept anonymous for confidentiality, explained that “one of my cases, they walked out of school and the police had to collect them on a 136 and take them to a suite, but there was no mental health beds to be admitted to and they definately couldn’t be free to go…so they were in the 136 suite for a week. It’s better than a&e, or nothing, but you’re only meant to be there for 36 hours maximum…it’s not for long term care.” The environment is unsuitable with agitated patients sat in “an old linen cupboard with two police at the door”, explained McKillop, and others trying to commit suicide within A&E8.
The NHS is experiencing a period of record demand and an understaffing, underfunding crisis11. The rising plea for mental health treatment and use of s136 falls on police to fill the unfortunate gap. In 2024, a review found police spend 800,000 hours annually waiting with MH patients2. When approached the Metropolitan Police revealed that their average involvement time between 2023-2025 was 12 hours per 136, occasionally stretching to 31 hours. “There is an excessive time spent dealing with Section 136 detentions”, former MH lead officer, Peter Weaver commented.
An increase of 8.4% in mental health contacts compared to the 7.2% increase in mental health nurses and health visitors suggests workforce expansion is not keeping pace to match demand12.
Officer Simon Cantrill outlined, “our training could always be better…if officers are forced to sit with a detained person in A&E, a vehicle outside a 136 suite or an over-flow room, the training isn’t good enough”. This, of course, is not always the case, Weaver continued that he felt his officers “dealt with them much better than mental health staff, more understanding, more empathy.” Investigating death or improper use of restraint during the MHA does not intend to blame every officer, especially as this goes beyond their job description, rather it is vital to identify patterns for the safety of individuals with mental health vulnerabilities.
Incidents where s136 has gone wrong have cropped up previously. Individuals have been punched during detainment13, others tasered and restrained14, and more recently found dead in a police van parked outside a hospital15. McKillop discussed her interaction, noting that “you get some who are really kind who say they are there because they want you to get help”. She seemed uncertain but added, “there are others that don’t want to be there…they’ll say we wish we’d just arrested you for taking our time, saying if we pick you up near a motorway we can charge you. The threats are constant but I’ve never been charged, it adds to the stress though, thinking I’m going to be arrested”. Another s136 detainee explained, “it is overall how you behave towards them. If you’re nice they show you respect, if you’re not they’re won’t”. She continued, “some won’t take the cuffs off for the 10 hours and when I need a drink I sit there and they pour water into my mouth. I’m not a criminal…my emotions are all over but I can have a drink of water myself”.
There have been cases involving s136 raising concern about race, for example, Kevin Clarke who was mentally ill and died following restraint despite exclaiming that he couldn’t breathe16. Existing incidents have led to laws introduced that hold training accountable for use of force with mental health17. It is not a policing function to support individuals for up to 3 days under section 136. However, where police powers are involved, it is essential to monitor the use of force to ensure no group, including ethnic minorities, is disproportionately affected…
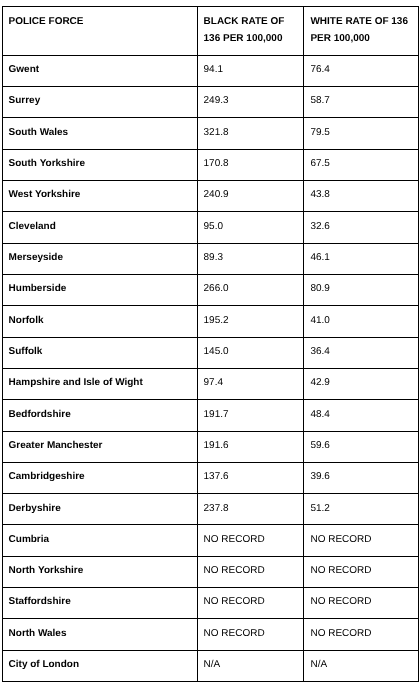
Black people were detained four times the rate of white people under the MHA, placed on a Community Treatment Order eight times the rate18, and following the pattern, 2.8x as likely to be detained under Section 13619. Black and ethnic minority people are seemingly more likely to access mental health support through the criminal justice system first, they meet police before clinical intervention20. Professionals have expressed their outrage that the system is failing Black people and urgent intevention is needed to address the worsening situation21. What can be done to address these issues? Mandatory training! The current mental health bill is weak22 in the face of deepening racism and the RCN cries for training specific to mental health and discrimination23.
Introducing PRAP! The Police Race Action Plan24, a great effort to solve racism within the police force. Established in 2022 it demands new training to be introduced that supports Black people with mental health issues.Overall, this will “develop a greater awareness of mental distress within Black communities to use that knowledge to improve policing interactions24.” (National Police Chiefs’ Council & College of Policing, 2022, pg. 45). So, we have a world where mental health demands are rising, police are first response, and Black people are disproportionally affected. Is PRAP a suitable cure?
No. Out of the forces spoken to for this investigation, none have implemented mental health training in response to PRAP to address the racial bias the Black community faces. In 2022 PRAP requested further training regarding mental distress and as of 2026, over 3 years later, this has not been done. Evidence from forces across England and Wales shows that PRAP weakly exists half-embedded into systems. Concerns have been previously raised that the money spent on PRAP has been on consultation, tick-box tasks without addressing racial disproportionality25, and here is the evidence of such…
Firstly, several forces outright confirm they have either no training in response to PRAP and all forces spoken to say they deliver no training for mental health for the Black community. To demonstrate, Bedfordshire police state there is ‘no official PRAP training material’ in response to a request for information. Similarly, Greater Manchester Police directly confirm there is ‘no specific training relating to the Police Race Action Plan’. This pattern repeats across each force - there is no trace. Further lacking, is evaluation, auditing, or any idea if the training that has been impletmentd since PRAP, non-specific to mental health, has been effective to combat racism. Surrey confirm they hold no data on who has completed training beyond new recruits and similarly Staffordshire state no evaluation or audits are held in information released, again a pattern repeats across forces.
This graph is based on counts of officer-observed ethnicity as this gauges how the police perceive the individual at first reaction. Self-identified ethnicity is not recorded by multiple forces. North Wales does not record ethnicity for s136 at all. Guidance suggests using self-identified for accuracy yet non-recording has increased in recent years4.
Where there are positive elements that address PRAP correctly, they come with a disappointing partner in tow. Merseyside police work with Anthony Walker charity and have trained 96% of their workforce together, this appears legitimate and successful, yet is undermined by the training being 2-hours long. Is this sufficient to address long-standing systematic racism? Similarly, North Yorkshire can be recognised for taking PRAP seriously, spending £124,000 on their programme that contains 63 full day sessions, yet it does not address mental health and they only aim for 78% completion despite being ‘mandatory’. Again, Humberside covers Black history in detail, has a podcast to discuss experiences, and officers visit places of worship to listen and learn. However, unfortunately, they reveal only 60 officers have completed the PRAP training out of a huge 2,300. Overall, the attitude towards mental health appears over-generalised and dismissive, failing to address the distinct experiences that lead Black people to be disproportionely detained under Section 136.
An image selected from Humberside’s released PRAP training
PRAP has faced scrutiny from the ISOB chair who felt the plan was so poor that it was either unheard of or not implemented in local forces correctly. Similarly, the National Black Police Association suspended support in 202427, and since re-engaged with no confirmed explanation. Jacob Henry, co-founder of Vibe Youth, previously on the panel for PRAP scrutiny, explained his reason for leaving when approached, “I did not feel that the space was leading to meaningful change or having the level of impact that was needed”. He speaks on behalf of the Black experience, noting with disappointment that he saw no “demonstration of how these initiatives are translating into measurable change”, and that another plan has been created “without a genuinely embedded commitment to systemic change”. The budget for PRAP has faced criticism28 for failing to spend a third of the overall budget since it was introduced. Although more money was spent in 2024/25, the allocated amount has been decreasing29 in the past two years despite the amount of training to be delivered, the funding does not reflect the miles left to go.
A system that cannot efficiently monitor who it detains, for how long, or where, is broken. Especially one that is underfunded with an underlying attitude of dismissal towards systematic racism. Section 136 is a point of crisis turned into exposure through watchful A&E audiences, police are the new mental health staff, and for Black people distress is unequally read as a threat. Section 136 will always be a necessity, but we must continue to observe the unwilling hands that deal out the trauma and to whom.